A general blood test can be called the most common clinical test that is taken in childhood and adulthood. Its indicators help to identify disturbances in the functioning of the body and diagnose many diseases.
Norm
Before you find out if the indicators are normal child analysis blood, you should find out exactly what indicators are determined and what they are responsible for.
What these between-group differences may mean for our understanding of the relationship between language and childhood stuttering will be discussed below. However, this finding can be compared with other studies in which GPA typically developing children up to school age on some of the most commonly used tests with rates higher than average. In addition, some language abilities in other groups of children have been shown to be preschool age significantly different from those of the control group, although both experimental and control groups scored within normal limits.
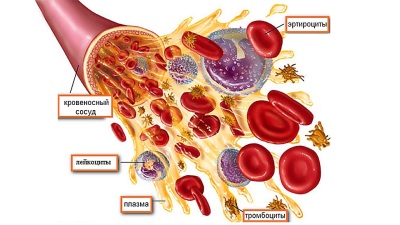
A general blood test determines:
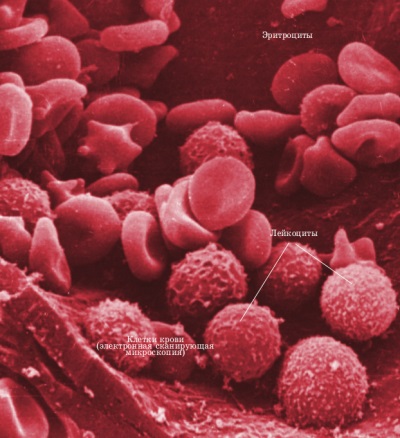
- This is the name of red cells, the most important function of which is the binding and transport of oxygen and carbon dioxide. The hematology analyzer additionally determines such parameters of red blood cells as distribution width (shows the difference between the largest and smallest cells) and average volume. Like the hemoglobin concentration in a red blood cell, these parameters are needed by hematologists to make a diagnosis different types anemia.
- Hemoglobin. It is a protein found in red blood cells that binds oxygen and also carbon dioxide. Its structure contains heme, which contains iron. It is due to the presence of heme that red blood cells and blood have a red color. The study determines how many grams of a given protein are in a liter of blood.
- Color index. A parameter calculated using a special formula that shows how much hemoglobin is contained in a red blood cell.
- Hematocrit This indicator determines how much of the total blood is made up of cells, that is, it indicates the thickness of the blood.
- Reticulocytes. This is the name of young red blood cells, the number of which is determined in ppm.
- These are white blood cells that help protect the child’s body from various infections.
- Leukocyte formula. This is the name given to the percentage of types of leukocytes present in the child’s body.
- Platelets. Such blood cells are important for stopping bleeding in the event of vascular damage. These cells are also called blood platelets because of their shape.
- ESR. This parameter shows how quickly blood cells settle, separating from the plasma.
![]() A general blood test shows the values of 9 indicators at once
A general blood test shows the values of 9 indicators at once
One possible explanation relates to the relationship between attention and development vocabulary, given that word learning involves the child directing his attention to words and their referents. Finneran et al.'s finding suggests that there may be a link between children's attention and receptive lexical abilities. Another possible factor in differences between groups in vocabulary is phonological working memory, which is thought to play a role important role in learning words. As with attention, we do not fully understand the possible contribution of phonological working memory to between-group differences in word learning and vocabulary development, but this may also be an interesting area to study in relation to childhood stuttering.
The leukocyte formula includes:
- Neutrophils (cells containing granules to fight bacteria), which normal analysis There are segmented (more mature neutrophils, represented in larger numbers) and band (younger forms). There are also such forms of neutrophils as young (metamyelocytes) and myelocytes. These forms are immature and appear in blood tests during diseases.
- The second group of leukocytes are eosinophils, which also include granules, but react not to bacteria, but to allergens.
- Basophils, which also have granules, are present in small quantities in the blood. In the hematology analyzer, the GRAN parameter is determined, which takes into account all granular forms of leukocytes (basophils, eosinophils and neutrophils).
- Large group Leukocytes are lymphocytes responsible for immune responses. They respond primarily to viral infections.
- Cells called monocytes engulf bacteria, dead cells and other particles that need to be removed from the body.
- And another type of leukocyte, present in very small numbers, is called plasma cells. They form antibodies.
Normal values for each indicator differ in at different ages child:
Alternatively, one could argue that since this meta-analysis of “speaker group differences” is primarily based on norm-referenced tests, the differences reported may be given rather than rater-specific. However, although this alternative explanation cannot be completely refuted, the results of other studies do not make it plausible.
There is some question whether the above-mentioned between-group differences in language ability contribute to the actual incidence of stuttering. To address this question, it is necessary to empirically evaluate the relationship between various language abilities and stuttering behavior across the various studies included in this meta-analysis. Unfortunately, this was not possible due to the fact that several of the studies reviewed provided insufficient information about stuttering behavior. However, refutation or support of such speculation must await further empirical research.
|
Red blood cells (1012/l) |
Hemoglobin (g/l) |
Color index |
Hematocrit (%) |
Reticulocytes (‰) |
Leukocytes (109/l) |
Platelets |
ESR (mm/h) |
|
Normal leukocyte formula:
Moderation of methodological factors in relation to differences between languages
For none of the five main analyses, results were moderated by methodological factors.
Possible clinical consequences
The present authors questioned whether language ability was related to childhood stuttering. This question has been answered, at least in part, in the affirmative, leading us to consider what role language may play in the assessment and treatment of childhood stuttering. Of course, it would seem that preschool and early school-age children known or suspected of stuttering should receive the same comprehensive evaluation for speech language received by other children with known or suspected speech language problems.|
Band neutrophils |
||||||||
|
Segmented neutrophils |
||||||||
|
Eosinophils |
||||||||
|
Basophils |
||||||||
|
Lymphocytes Shift formula leftThat is, focusing on the fluency of a child known or suspected of stuttering, especially when the initial “diagnosis” comes from casual or casual listeners, may distract the clinician from simultaneously considering other, significant aspects of speech ability and development. In some cases, as recent research shows, such an assessment can reveal underlying problems speech speech that must be taken into account when developing comprehensive plan treatment for the child. Whether such an assessment reveals an overt language disorder, normal but below typical language abilities, or neither, consideration of language associations with childhood stuttering should help in language processes can only broaden rather than narrow our basic, as well as an applied understanding of this childhood disorder. |
||||||||
|
Monocytes |
||||||||
|
Plasma cells |
Reasons for deviations
Each indicator general analysis blood is analyzed separately.
When the number of red blood cells is low, anemia is diagnosed. Its causes may be blood loss due to injury, a diet poor in proteins and vitamins, fermentopathy, leukemia or death of red blood cells due to hemolysis.
Uncontrolled Variables: Nonlinguistic Measures
Additionally, some of these studies used fairly small samples. Therefore, findings related to some areas of language development, as mentioned above, are more suggestive than conclusive.
Uncontrolled Variables: Language Measures
To be included as a participant, children must not have scored within the normal range on norm-referenced tests of language development. The absence of this inclusion criterion applies to both groups, indicating that both speaker groups have an equal opportunity or probability of including participants who score below normal limits.An increase in the number of red blood cells may indicate dehydration, erythremia, renal artery stenosis, as well as diseases causing cardiac or respiratory failure.
 A deviation of the red blood cell count from the norm indicates problems in the child’s body.
A deviation of the red blood cell count from the norm indicates problems in the child’s body.
The present results were primarily based on norm-matching tests and spontaneous language samples. Thus, future empirical efforts to examine differences in language differences between conversation participants described in the present study may benefit from implementing research methodological approaches that are familiar with the literature on language and disorders but novel in the field of childhood stuttering research.
To do this, a systematic identification, integration and synthesis of a population of 22 studies that met several suitable, seemingly stringent inclusion criteria was carried out using meta-analytic procedures. Equally important, differences between language differences between groups cannot be explained by methodological differences between various studies, making reports of differences in language ability even more reliable.
Hemoglobin
Low hemoglobin levels are also diagnosed as anemia, which can be caused by poor nutrition, blood loss or congenital blood diseases.
If hemoglobin, on the contrary, is elevated, the causes of this condition may be dehydration, kidney, lung or heart disease affecting blood flow, as well as erythremia.
This research was supported in part National Institute of Health, awarded to Vanderbilt University. The authors would like to thank Dr. Melanie Schule for providing her with scientific information, leadership and commitment to the development of this study. Jones for inter-judge reliability of measurements. References marked with an asterisk indicate studies included in the meta-analysis.
Age of onset and repetition apply effects to depictions of children who do and do not stutter. Language abilities of children who stutter: An exploratory study. Structural ranking scheme for young children who do and do not stutter.
Changing the color index
The parameter will be increased with erythremia, heart failure, dehydration, and respiratory failure.
Its decrease is observed in anemia and renal failure.
An increase in the number of white blood cells (leukocytosis) may be physiological. Such leukocytosis occurs for several hours after eating, and also for some time after physical activity(in infants after prolonged crying) or emotional overload.
Increase in the number of red blood cells
Linguistic variables in childhood stuttering: Speech dissociations. Thermal characteristics of young people who stutter. Unique repetition skills in young children who do and do not stutter. Developmental deficits in short-term phonological memory: Implications for language and reading.
Wichita State University; Kansas: Analysis of the metalinguistic behavior of children who stutter: Kindergarten through second grade. Irregular word production in children who do and do not stutter and conceal the repair hypothesis. Analysis of children's language: methods and theories.
 An increased number of white blood cells in the blood may be temporary
An increased number of white blood cells in the blood may be temporary
A pathological increase in leukocytes occurs when:
- Purulent-inflammatory diseases;
- Oncological processes, including leukemia;
- Injuries and burns if damaged big square bodies;
- Exacerbation of rheumatism;
- Postoperative recovery.
A decrease in the number of leukocytes (called leukopenia) is noted with:
Californian State University; Long Beach, CA: Selected linguistic variables and their associations with stuttering and normal dysfunction in stuttering and non-stuttering preschoolers. Stuttering: A psycholinguistic perspective. The nature and treatment of stuttering: new directions. The effects of gradual increases in sentence length and complexity on the absence of children.
Parental perception of child communicative development at the onset of stuttering. Some empirical observations about early stuttering: possible relationship with language development. Introduction to meta-analysis. Repetition repeated word and receptive vocabulary for children younger age: A longitudinal study.
- Infectious and viral diseases;
- Systemic lupus erythematosus and rheumatoid arthritis;
- Some forms of leukemia;
- The use of steroid drugs and cytostatics in the treatment of tumors;
- Hypovitaminosis;
- Radiation sickness.
Leukocyte formula
|
Type of leukocytes Rapid learning of incidental verbs in 4-year-olds: Identification and generalization. Unpublished doctoral dissertation. University of Iowa; Iowa: The roles of syntactic and prosodic components of grammar in early childhood stuttering. Sentence position and syntactic complexity in early childhood stuttering: A longitudinal study. Expressive and receptive language skills in children who stutter. The role of phonology in childhood stuttering and its treatment. Stuttering and related disorders. Proceedings of the Third World Congress on Infertility. University of Pittsburgh; Pennsylvania: Comparison of Children's Stuttering Rates in kindergarten and the effectiveness of non-statistics on tasks of metalinguistic consciousness. Childhood stuttering and dissociation across linguistic domains: Replication and extension. |
What does the increase indicate? |
What does a decrease indicate? |
|
Neutrophils |
|
|
|
Eosinophils Temperament: Comparisons between children who stutter and children who do not stutter. Proceedings of the Third World Convention on Fugitive Disorder: Theory, Research, Treatment, and Self-Help. Nijmegen, The Netherlands: University of Nijmegen Press; P. 557-. University of Iowa; Iowa: Language measures of stuttering and nonintegrating children. Differences in repetition rates of children with and without specific language impairment: A meta-analysis. Moderate regulation in young twins with probable stuttering, high non-essentiality, and typical fluency. Sustained attention in children with specific language impairment. Repetition intrusion and word learning: The nature of the relationship. Phonological short-term memory and vocabulary development: Further evidence of the nature of the relationship. Monocytes Basophils |
|
|
|
Lymphocytes |
|
|
Separately, it should be noted the distribution among the forms of neutrophils:
Young children and adults use lexical principles to learn new nouns. Diagnostic accuracy and test-retest reliability of repetition and gap repetition tests for preschool-age children with specific language impairment.
Is there a relationship between the development of cognitive-linguistic abilities in children and the progression of stuttering? Distress disorders: theory, research, treatment, and self-help. Reproduction of irregular repetitions in children who stutter: A study.
Lexical development and retrieval in the treatment of children who stutter. Language learning in childhood stuttering. Stuttering and airless disorders. Effect size estimates from a series of independent experiments. Attentional functions in speech disorders.
- If more band neutrophils are determined in the child’s blood, and myelocytes and young neutrophils are also detected, the leukocyte formula is interpreted as a “shift to the left.” It is characteristic of inflammatory and infectious diseases, acute blood loss, and intoxication.
- If the number of segmented neutrophils increases, this formula is called a “shift to the right.” Such an analysis may indicate a lack of folic acid or vitamin B12.
Platelets
The number of platelets will exceed the norm if the child has had the spleen removed or had any other operation, as well as with physical fatigue, erythremia, cancer, anemia and inflammatory processes.
If platelets are lower than normal, this may indicate hemophilia, heart failure, various infections, or aplastic anemia. Also, the platelet count may decrease after a blood transfusion, with disseminated intravascular coagulation syndrome and hemolytic disease in newborns, in premature babies, and after taking certain medications.
ESR
The indicator decreases very rarely, but its increase is often evidence of an inflammatory process in the body.
E. Komarovsky’s opinion on blood testing
A well-known pediatrician calls a blood test the ideal test because it quickly and cheaply provides answers to diagnostic questions. He finds qualitative and quantitative determination of the state of blood cells very informative.
 Blood test is effective analysis and allows you to identify many diseases
Blood test is effective analysis and allows you to identify many diseases
What to consider?
First of all, moms and dads need to remember that the child’s blood test results will differ from the norms established for adults. And if you were given a results form, the norms that are usually indicated on such a form apply to adults. So you shouldn’t panic if you notice a large deviation in the numbers.
The test results may differ depending on the time of day and depend on the child’s nutrition, so it is traditionally recommended to take the test at morning time on an empty stomach, but this is not a mandatory measure, but rather a wish.
You should also know that blood tests do not always determine all the indicators described above. Sometimes there is no laboratory assistant (without him the leukocyte formula cannot be determined), sometimes there is no equipment or reagents, sometimes the laboratory is overloaded. Mandatory indicators that are always determined are the amount of hemoglobin, the number of leukocytes and ESR.



